Presented by Steve Warfel, PT, DPT, MTC, CFMT, FFMT, FAAOMPT
Concussion or brain injury result from an impactful force upon the cranium or whip motion that comes to a sudden arrest. Both injuries have the same result, collision of the skull with the brain. Fortunately, the brain has multiple layers of protection, but what happens when any of these layers are compromised can change the entire system. In reviewing the literature, I was shocked to see the statistics!!! Approximately 5.3 million people in the United States are living with impairment in daily life due to either transient or long term neurological deficit resulting from concussion. Research has also shown that immediate diagnosis is very important. Patients with delayed concussion diagnosis have reported significantly increased symptom severity compared to patients who were immediately diagnoses.
So the first question is, how do I know if I have a concussion? Trauma induced concussions are often times related to the body’s ability to react. Let look at two examples. The mountain biker that flips over the handlebars and knows they are going to hit the ground has a chance to lessen the blow to the head and protect. He is also wearing a helmet that has the ability to absorb the shock of the impact internally. The impact is dispersed through the head, neck, and shoulder. No concussion. The second example is something that happens far too often in the winter. A pedestrian is walking down a snowy sidewalk and there is a patch of ice under the snow. She slips fall directly on her back and hitting the back of her head. At first she feels OK, just scared with how fast she fell. An hour later she begins to get a headache and become nauseous, and hour after that dizziness and vomiting. BAD CONCUSSION.
Immediate management is vital to successful outcomes when it comes to head injury or concussion. Case two above was taken to the hospital immediately and was found to have a mild brain bleed. She was kept overnight in the hospital for observation and then released to monitored care at home. Had she not sought immediate medical care the bleed could have progressed, leading to more damage or even death. It is so important to seek immediate medical care if any of the following symptoms present. Dizziness, double vision, difficulty walking or moving, disruption in speech or comprehension, light or sound sensitivity, nausea or vomiting, acute personality change, amnesia. These are the more obvious symptoms of concussion.
Now what about case one? The rider had no symptoms after the injury except lacerations on the face and a sore neck. The helmet did break, suggesting there was certainly impact to the head. A week later he started to have disruption in sleep and feel a little fatigued and irritable. Wisely, he decided to have a physical therapy evaluation. Despite the lack of cognitive, balance, visual, audio, or sensory deficit, his therapist found considerable dysfunction in the cranium, that when treated restored the rider’s normal respiratory rhythm. One treatment later sleep cycles were restored to normal. Had this individual continued with these symptoms, he may have progressed into adrenal fatigue, chronic fatigue, or depression among many other symptoms that can result from unmanaged head injury or concussion. The moral of the story here: Even if symptoms are very mild, see a medical professional to be sure they are managed correctly immediately.
What can be done when head injury or concussion heals and symptoms are not resolved? Many medical treatments are designed to teach the patient to habituate to the changes that have occurred, not correcting these changes. These clients are often “stuck” with pressure imbalance in the cranium. Cranial pressure must maintain homeostasis, which for a supine adult is 7-15mmHg. If there is a compression in the system there must be an equal and opposite expansion to maintain these pressures to assure there is no compromise in the cranial airway, sinuses, nervous system, brain, and vasculature. Emergency situations arise as ICP progresses over 20mmHg. Changes to the skull itself of the support membranes of the brain result in imbalanced pressures within regions of the brain. For example, a hit to the back of the head compressing the occipital bone in the base of the skull will force pressure forward into the frontal area of the skull.
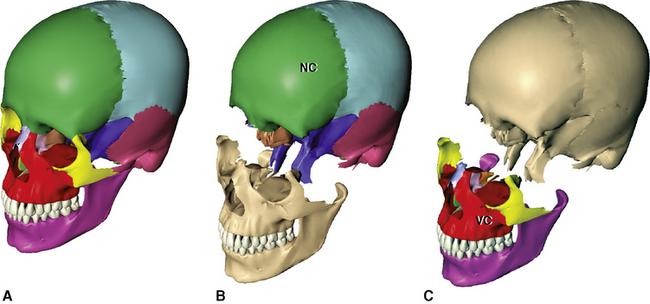
The skull is composed of 8 bones in the neurocranium (head) and 14 in the facial skeleton. Held together by fibrous inter-cranial sutures that begin life as very flexible structures to allow growth and shock absorption for the brain. Certain areas of the skull feature thicker bone designed sustain impact: frontal and occipital bones, zygomatic arches, maxilla. Other areas are paper thin and fragile: temples, nasal bone, lateral sphenoid. Impact to the skull can create imbalance within bony structures. The cranial bones can be treated and alignment restored via the cranial sutures or junctional zones between the bones. It is essential to restore the correct osseous structure, then the support membranes of the brain can be addressed.
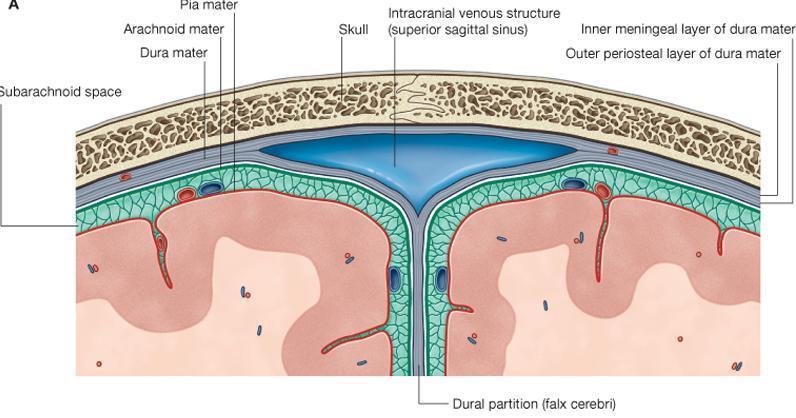
The brain features three structural membranes that secure it in the skull and bathe in cerebrospinal fluid. Along with blood, cerebrospinal fluid is vital for brain nutrition, waste elimination, shock absorption, and communication with the system. The first of these membranes is the dura matter, the toughest, outer most layer of the nervous system, functioning to protect, enable circulatory exchange, and support the cerebrospinal fluid system. The dura forms several vital support structures for the brain. The dura is a hood over the brain that forms into a tube that surrounds the spinal cord, traveling to the terminal nerve branches in the sacrum. The tentorium cerebelli is an extension of the dura that separates and supports the occipital lobe of the brain from the cerebellum, and stabilizes the cranial sinuses. The tentorium travels from the transverse ridge of the occipital bone to the petrous portion of the temporal bone and the clinoid process of the posterior sphenoid. The tentorium is a diaphragm, functioning like a tightly woven trampoline under the brain, absorbing shock and distributing cerebrospinal fluid. The tentorium works in sync with the respiratory diaphragm to set respiratory and cerebrospinal rhythms essential for proper sleep and neurological well-being. Finally, the falx cerebri is a longitudinal extension of the dura that separates and supports the hemispheres of the brain, and stabilizes the cranial sinuses. The falx is anchored anteriorly at the crista galli in proximity to the cribriform plate and frontal sinus. It traverses posteriorly following the mid sagittal suture, connecting terminally with the cerebellar tentorium around the internal occipital protuberance. The falx divides the brain hemispheres, providing fluid and neurological exchange between the two as well a shock absorption.
If there is compromise to any of these three membranes the effects on the brain are catastrophic. A decrease in profusion of cerebrospinal fluid immediately disrupts the respiratory and nervous systems. Fortunately, each of these membranes can be treated via specific pressure designed to redistribute cerebrospinal fluid. The goal of treatment is to identify where pressure is stuck in the cranium and where that pressure is being pushed to. Once these areas are discovered, light into the restricted area will start to draw pressure in from the over pressured area. The sooner after injury these techniques can be performed the better. The longer dysfunction remains in the cranial system, the longer it takes to resolve.
The other key area to be addressed with head injury and concussion is the circulatory system. The brain has an incredible capillary network that assumes the shape of the brain and face! When trauma occurs, there is damage to these micro vessels that leaves the corresponding area of the brain with a little less circulation, or difficulty draining blood, leaving pressure in the cranial vault. This treatment approach focuses on treatment to the heart and carotid arteries that supply the brain to improve the efficiency and output of the cardiac system. Both result in irrigation to the smaller vessels and revascularization of neural tissues. Nerves like everything else in the body need blood to survive and heal. Circulation is often lacking in often lacking in unresolved concussion. Restoring blood can result in restoration of neural function regardless of the injury or how long it has been present.
My goal in writing this blog was to educate as many people as I can on a topic that affects so many. I also want to inspire hope in the 5.8 million people who are dealing with daily functional limitation due to impaired brain function post-concussion…….THERE IS HOPE!!!! If you know someone who if suffering with any degree of symptoms, please share this with them. All of us at KinetiChain treat the cranium and would be happy to help. I will also attach several resources below. IAHP- a group that offers Craniosacral treatment via the Upledger Institute and Neuromeningeal Manipulation via the Barral Institute. The other is the Institute of Physical Art- a group that offers an approach called functional manual therapy. Looking for a highly trained practitioner is essential as not many have training in cranium. Please contact me directly with any feedback or questions at [email protected].